

Why Medicaid Cuts Will Cost More Than They Save
Plus The Hidden Cost of Medicaid Work Requirements


It’s a short week so we are coming to you with a joint piece on the recent BBB or “Big Beautiful Bill” and the adverse impacts it will have on millions of Americans.
Recently, the House has advanced budget proposals that would significantly cut Medicaid spending in the name of deficit reduction. House leaders have instructed committees to find $880 billion in Medicaid savings over 10 years – an enormous reduction given that Medicaid covers about 72 million Americans (nearly 1 in 5). Since top GOP officials (including President Trump and Speaker Mike Johnson) vowed to spare Medicare and Social Security from cuts, Medicaid has become the prime target. The focus is on trimming coverage for working-age adults, a group many conservatives frame as less “deserving” than seniors – but working-age adults in rural areas are especially likely to rely on Medicaid, which makes these cuts particularly thorny.
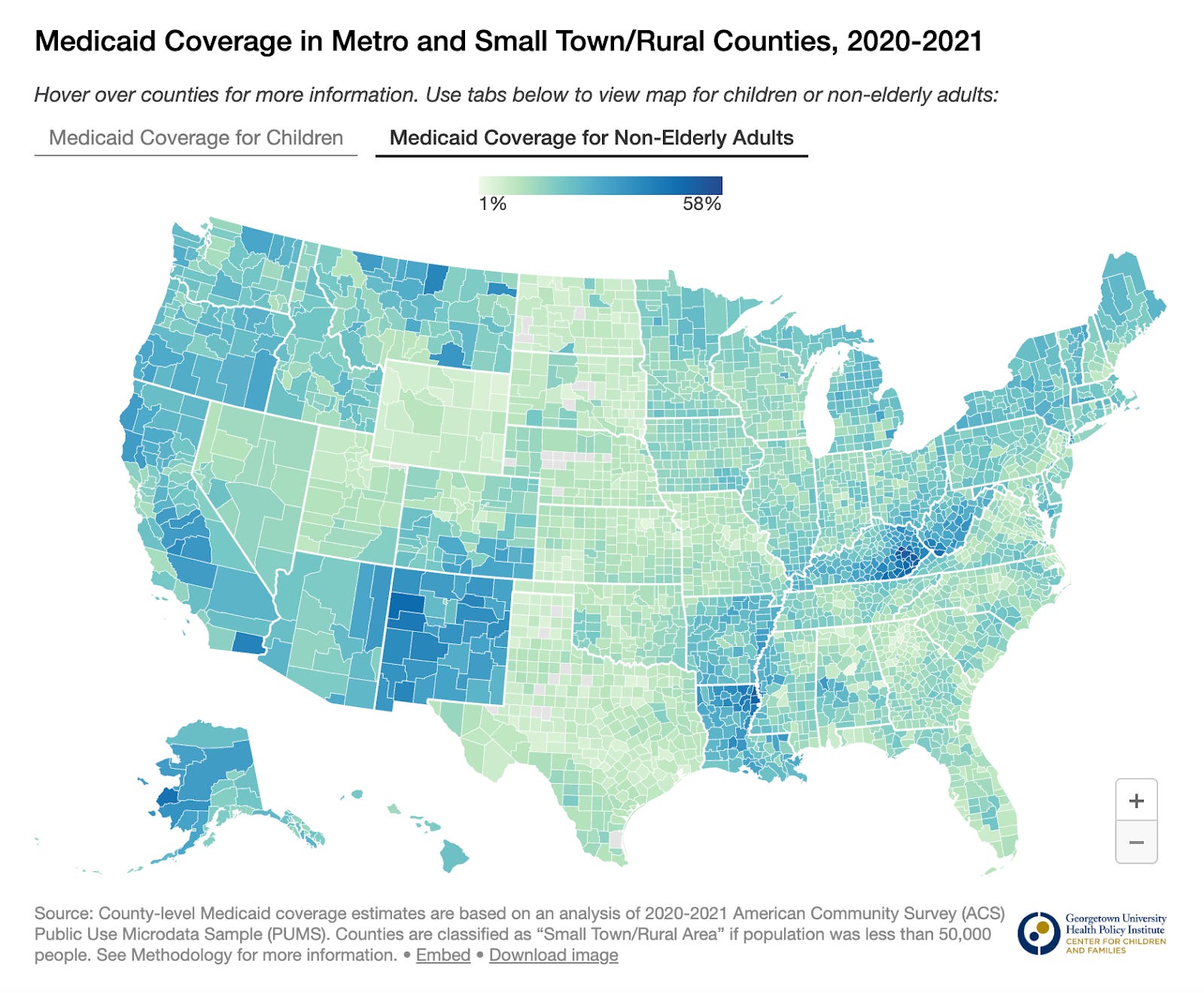
Image Credit: Georgetown University Center for Families and Children.
Several specific legislative proposals have emerged. One idea would roll back the Affordable Care Act’s Medicaid expansion by reducing the federal funding match from 90% down to the standard rate (around 50–77% depending on the state). KFF estimates this change would slash federal spending by $626 billion over a decade. Crucially, nine states (including North Carolina, Montana, Indiana, and others) have “trigger” laws to automatically end their Medicaid expansion if the federal match drops. In other words, millions could lose coverage overnight. Another proposal is to impose work requirements on “able-bodied” Medicaid enrollees. The Congressional Budget Office projected that a nationwide work requirement (such as 80 hours of work, job training or volunteering per month) would save around $109 billion in spending over 10 years, but by ultimately leaving about 600,000 people without health insurance. (Other analyses suggest even larger losses of coverage: roughly 1.5 million people would lose Medicaid eligibility under the House’s work requirement.) Yet proponents of work requirements persist in promoting a policy that sounds reasonable in political terms “People should work for it!” but crumbles in implementation, failing to achieve its intended purpose, while harming millions.
The Myth of “Work to Deserve” Care
House Republicans want to add work requirements to Medicaid, cutting off coverage for childless adults who can’t prove 80 hours of monthly employment. The idea is that people should “earn” their benefits, but the policy is both cruel and ineffective.
As Matt Bruenig wrote, these rules punish people for things beyond their control. Employers, not workers, decide hours, hiring, and layoffs. Over 20 million people are fired or laid off each year, and many low-wage jobs have unstable hours that make hitting the 80-hour mark difficult, even for the employed.
When Arkansas tried this in 2018, 18,000 people lost Medicaid within four months, but employment didn’t rise. The only clear result was more uninsured people.
The myth of the “freeloader” doesn’t match reality. Just 6% of working-age Medicaid recipients aren’t working long-term, only 3% of the total Medicaid population. Meanwhile, 48% are employed and another 27% are disabled. These rules don’t target laziness; they hit the vulnerable.

Image Credit: The New York Times
In practice, work requirements act as paperwork traps. When COVID-era protections ended, nearly 70% of disenrollments were due to paperwork issues, not eligibility. Adding more red tape will push people off coverage for failing to navigate bureaucracy, not for refusing to work. As Benjamin Sommers, a professor of health policy who has studied Medicaid work requirements notes “This is not savings through improved efficiency, or more people going to work. It’s savings by kicking people out of the program who are mostly eligible.” For some lawmakers, that may be the goal.
As Bruenig asks: “We don’t deny fire or police services based on someone’s work hours. Why would we deny medical care?” Medicaid is meant to be a safety net, not a reward for stable employment in an unstable economy.
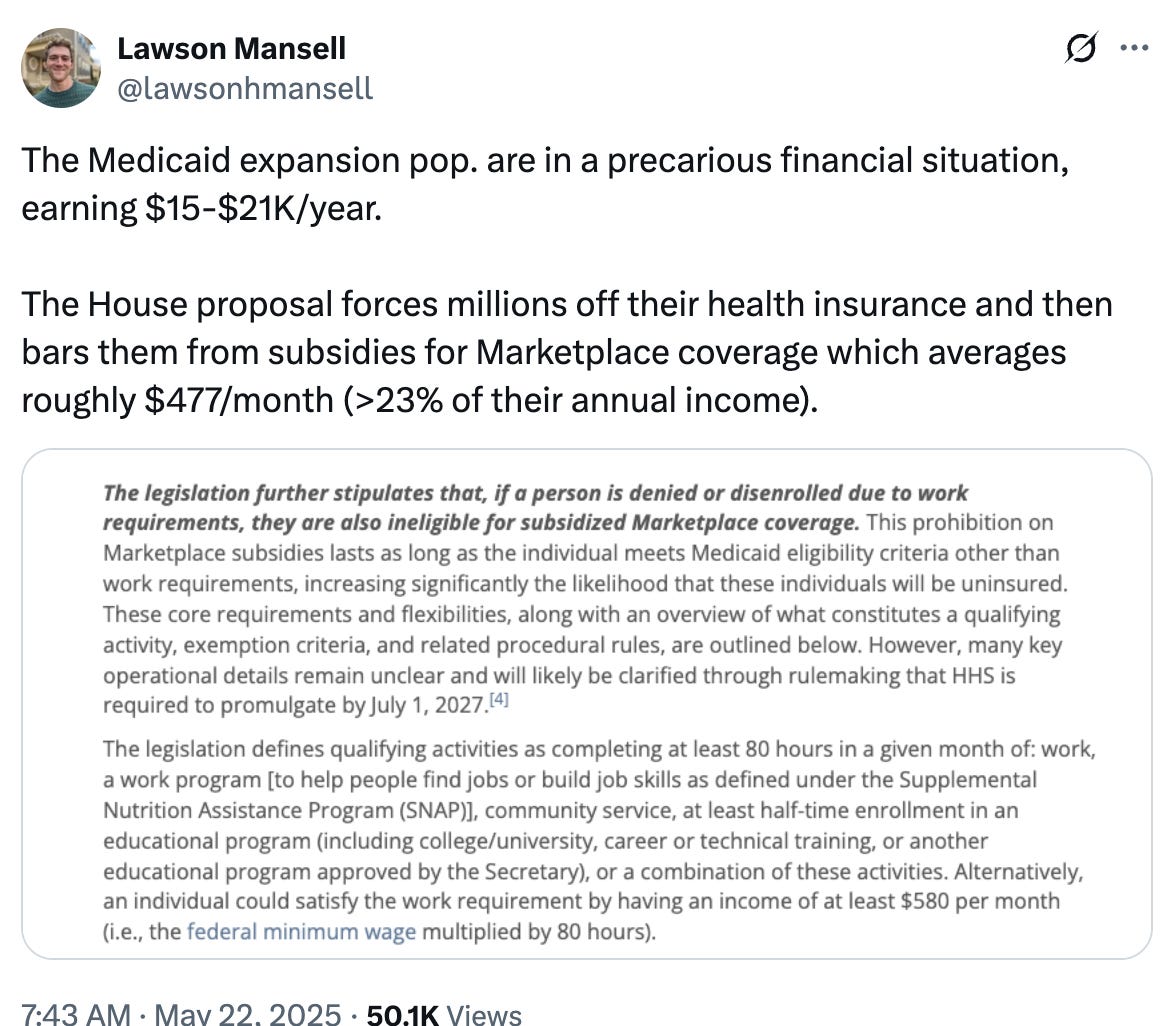
Under the proposal, individuals kicked off Medicaid for failing to meet new work requirements would also be barred from receiving subsidized Marketplace insurance. That means someone earning just $15,000 to $21,000/year (typical for many Medicaid expansion enrollees) would be forced to pay over $477/month for a basic health plan, more than 23% of their annual income.
It’s a deliberate catch-22: people too poor to afford unsubsidized insurance are disqualified from free coverage unless they can prove consistent work even though low-wage jobs are often unstable and schedules unpredictable. This isn't about encouraging work. It’s about reducing the Medicaid rolls by making eligibility so restrictive and punitive that people fall through the cracks.
When people lose Medicaid coverage, they don't simply stop needing healthcare, they're forced into a brutal financial bind. Without insurance, routine medical visits that Medicaid would cover for free suddenly cost hundreds of dollars out-of-pocket. For someone earning $15,000-20,000 annually (common for Medicaid expansion enrollees), even a single medical emergency can trigger financial catastrophe. The cruel irony is that delayed care often leads to more expensive interventions later; untreated diabetes becomes diabetic ketoacidosis requiring ICU admission, ignored chest pain could become a massive heart attack, and routine infections may become life-threatening sepsis.
The Reverse Robin Hood
Rural Americans will bear a disproportionate burden from these Medicaid cuts, facing a perfect storm of geographic and economic vulnerabilities. The damage extends beyond individual patients to entire healthcare systems. Rural hospitals, already operating on razor-thin margins, depend heavily on Medicaid reimbursements to stay afloat. When patients lose Medicaid and can't pay for care, hospitals absorb these costs as uncompensated care, pushing many toward closure. Between 2010 and 2021, 136 rural hospitals closed. 700 more, a third of all rural hospitals, are in danger of closing in the near future. Medicaid cuts could accelerate this trend dramatically.
For rural residents, losing the local hospital means traveling hours for necessary care. The economic spillovers are devastating. Rural hospitals are often among the largest employers in their communities, and closures eliminate hundreds of jobs while eroding the local tax base. This creates a downward spiral where healthcare cuts trigger broader economic decline, making rural communities even less viable and further widening the urban-rural divide that already plagues American politics. Republicans’ Medicaid cuts aren't just going to hurt the most vulnerable people; they’re going to hurt the most vulnerable places.
It’s also worth pointing out what all of these cuts are in service of. It’s not reducing the deficit. Republicans’ Big Ugly Bill would increase the deficit by $1.7 trillion according to the Tax Foundation. Instead, it’s about giving tax cuts to wealthy people who do not need them. At the end of the day, giving a tax cut to rich people is a bad idea from a deficit math standpoint and giving that tax cut while cutting healthcare for vulnerable people is outrageous from a moral standpoint.

Image Credit: Center on Budget and Policy Priorities.
Scarcity vs. Abundance: Rethinking the Health Care Equation
Finding ways to deny vulnerable people healthcare is the wrong way to think about healthcare economics. As the Niskanen Center argues, the U.S. healthcare system suffers from a fundamental imbalance between demand and supply. We have an ever-rising demand for care (an aging population, new treatments, etc.) constrained by relatively fixed or slow-growing supply (doctors, clinics, drugs) – a recipe for high prices and limited access. In fact, America spends more on health care than any other OECD country yet has some of the worst outcomes (like the highest rate of avoidable deaths). This suggests that simply pouring more money into the existing system (or conversely, slashing funding for patients) won’t solve the core problem. Instead, reformers are increasingly talking about “healthcare abundance” – the idea that we should focus on expanding the supply of healthcare so that it’s plentiful and affordable, rather than rationed by price or bureaucracy. As with the YIMBY approach to housing, the core insight here is that you can’t redistribute your way out of a shortage.
Healthcare abundance offers a different path: increase the overall capacity and productivity of the health system. In practical terms, that means investing in the supply side, more providers, clinics, technologies, and innovations, and removing the barriers that artificially constrain supply. Instead of viewing healthcare as a zero-sum budget game, an abundance mindset asks how we can make more care available to more people at lower cost by unleashing competition and creativity. This could reconcile the goals of both sides: protect patients from crushing costs and control government spending, not by denying care but by making care cheaper and more efficient to deliver. It’s analogous to how other industries became more affordable over time, through innovation and scaling up supply, not by telling consumers to make do with less.
Real fiscal responsibility means investing in solutions that work for everyone. Instead of asking "who deserves care?" we should be asking "how can we make quality healthcare accessible and affordable for all Americans?" The answer lies not in cutting coverage but in expanding capacity; training more healthcare workers, building more clinics, removing regulatory barriers that constrain supply, and fostering the kind of innovation that has made other essential services more affordable over time.
Healthcare is not a zero-sum game. We don't have to choose between fiscal discipline and human compassion.