

The Healthcare Regulation Everyone Should Hate
Certificate-of-Need Laws Raise Prices, Reduce Access, and Increase Mortality


For years, opioid addiction has ravaged communities across this country. Getting addiction treatment can be a matter of life and death for patients. In Shelby County, Alabama, a few towns over from where I grew up, Longleaf Recovery wanted to build a new 60-bed addiction treatment facility. Important fact: Alabama only has about half of the number of addiction recovery beds per capita as the national average.
Seems pretty straightforward, no? A medical service provider wants to provide an important service so you’d think the government wouldn’t stand in the way. Not so fast. Alabama, like 34 other states, has what are called certificate-of-need laws (I’ll explain those in a second) and Alabama’s certificate-of-need law covers addiction treatment. Meanwhile, in Alabama, Bradford Health Services operates most of the state’s addiction treatment recovery beds. They don’t want competition. So, when Longleaf has gone before Alabama’s Certificate-of-Need board, Bradford has filed formal challenges with the board, essentially blocking Longleaf from building their new facility. There are people suffering from addiction who could have gotten treatment at Longleaf’s facility, but they couldn’t because of the way this CON law blocked competition.
This is not a one-off weird mishap in one corner of the country. 35 states have certificate-of-need laws, and they cause widespread damage. Marianne Proctor, a Kentucky legislator who is working on CON law reform, recently said “I just don’t think many people know what it is.... If there were a way to explain it in a simpler way, I think people would have their hair on fire.” She’s right. So let me explain them in that simpler way. We’ll see if your hair is on fire by the end.
The best way to understand certificate-of-need laws is with a thought experiment. Imagine you wanted to open a new Mexican restaurant, but there’s a law saying you first have to prove there’s a need for Mexican food in your area. You’re confident there’s demand but proving it would be tough. Now imagine the board you appear before is mostly made up of local Mexican restaurant owners — and other restaurant owners can formally object to your application. Imagine also that the only way to get past their opposition is to agree not to encroach on their business — like promising you won’t stay open past 8pm. And finally, imagine the board can deny your application if you ‘duplicate’ an incumbent’s offerings. There’s a taco stand nearby that sells carnitas? No pork on your menu then.
This sounds insane, right? Well, that’s what Certificate-of-Need (CON) Laws are doing in health care in the states that have them. Even as they fail to accomplish their stated goals, they raise prices and make it more difficult for people, particularly in rural areas, to access needed healthcare services.
The Barriers to Competition That CON Laws Create
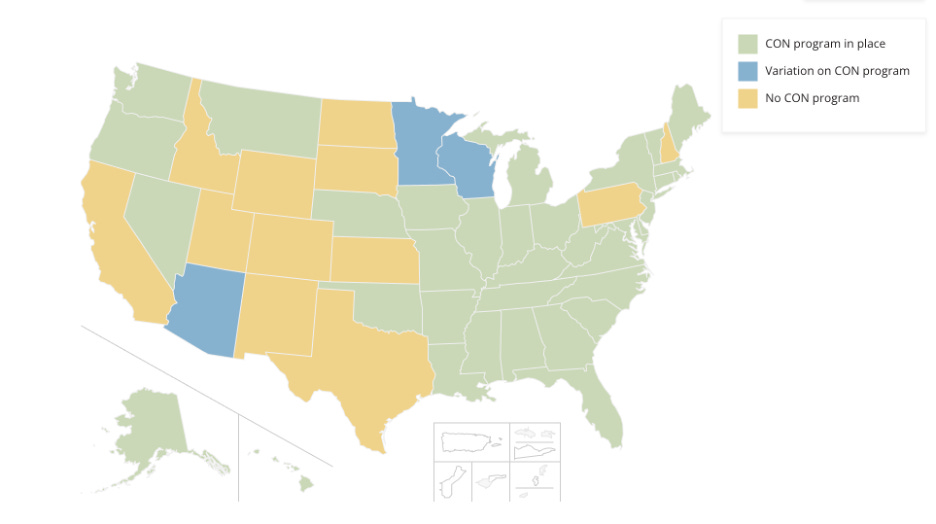
Several states have repealed their CON laws over time. Still, 35 states have a CON law in place for at least one medical service. The extent and rigor of these laws varies. Six states have CON laws for only one medical service (Montana’s only CON law for example is for long-term care facilities), but 22 states have them for 15 or more different kinds of medical services.
As in our Mexican restaurant thought experiment, in states with CON laws, would-be new medical service providers must go before a board and prove that there is a need for their service in order to acquire that ‘certificate-of-need.’ Employees of incumbent providers are frequently allowed, and frequently do, sit on these boards. In all but six states, incumbent firms are allowed to object to the application of their nascent competitor. CON laws typically require those boards to deny the certificate if the would-be provider is going to ‘duplicate’, i.e. compete with, a service already being provided by an incumbent. Some CON laws also require that a new service provider obtain a transfer agreement with an existing hospital; while that makes sense in certain circumstances, it creates yet one more way that incumbents can block the establishment of a new provider in their area.
The Cost to Patients
There is no telling how many would-be providers never even apply for a certificate-of-need because they know that they will never get through the process. The breadth of evidence that these laws raise costs is nevertheless staggering. CON laws are associated with:
On top of these cost problems, CON laws have significant adverse effects on access and patient outcomes. Compared to states without CON laws, states with CON laws have:
More post-surgery complications and worse readmission rates,
Higher mortality rates for heart attacks, respiratory disease, diabetes, COVID-19, and Alzheimer’s.
Each one of these findings is worth stopping to dwell on. The 30% fewer rural hospitals means towns losing their only emergency room (and that is compounded by the OBBB’s Medicaid cuts). The fewer imaging services means patients waiting weeks for an MRI instead of being able to get one that day. The higher mortality means real, non-theoretical people losing their loved ones. The scale and breadth of harm here in exchange for zero or near-zero benefit is, frankly, an outrage.
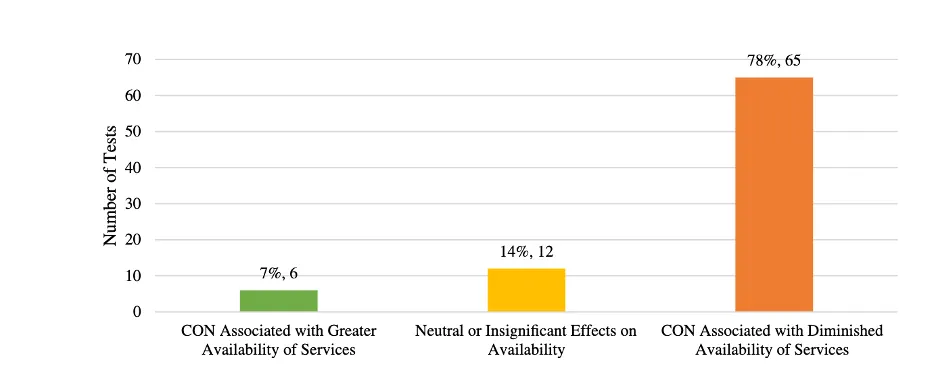
These are not cherry-picked results. Of 83 statistical tests done by researchers on CON laws, just 7% find an association between CON laws and greater availability of services while 78% of them find that CON laws are associated with diminished availability of services. CON laws don’t make sense to keep. Getting rid of them will not fix all of American healthcare but it will lead to more competition, better health care services, and lower prices.
The Good News
Fortunately, a number of the states that have CON laws are considering reducing them. Lawmakers in several states including Virginia, Hawaii, Georgia, Alabama, West Virginia, and Mississippi have introduced bills to create more exemptions to their CON laws or eliminate them entirely. Seven other states (Delaware, Rhode Island, Alaska, Iowa, Nebraska, South Carolina, and Tennessee) have informed the federal government that they plan to do the same. New Jersey recently passed a bill to expand its exemptions to CON laws. With luck, these and other states will reduce or repeal their CON laws. This would be a very pro-Healthcare Abundance set of reforms. It would remove regulatory barriers that make essential services artificially scarce and expensive. It would mean more doctors, more competition, lower costs, and better access.
-GW